Headshaking in horses

Headshaking has been well described as a syndrome for many years but is still a largely misunderstood condition.
Share this advice
It is of course, completely normal for a horse to shake his or her head. However about 4% of the UK equine population shake their heads more than normal. There are many reasons why a horse might shake more than normal, including dental problems, sinus pain and poor riding. However, by far the most common cause is a condition called idiopathic trigeminal-mediated (TGM) headshaking.
What is TGM headshaking?
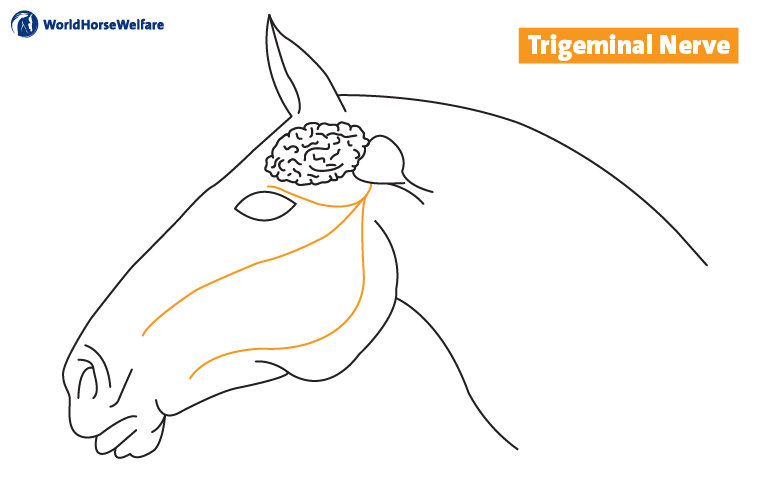
This is when the trigeminal nerve, the main sensory nerve to the face, appears to become some 10 times more sensitive than normal. We do not know why or how this occurs, with the nerve looking normal under a microscope. There is a complex association with environmental conditions, which is not understood, but does not seem to be allergy. The sensitised nerve appears to result in neuropathic (nerve) pain of the horse’s face. People with neuropathic pain describe varying intensity and frequency of burning, pins and needles and electric-shock like pain.
What are the clinical signs (symptoms)?
Horses with TGM headshaking usually show very classic clinical signs. These are of predominantly vertical headshaking, accompanied by sharp, vertical tics. This headshaking is accompanied by signs of nasal irritation, such as snorting, sneezing, rubbing the nose and even striking at the nose with the forelimbs. Signs can be present at rest but are usually worse at exercise and this is any exercise, not just ridden work. Signs can vary day on day and even by season by season, due to the environmental interaction. It can mean the horse cannot do his or her intended job and they can become dangerous to ride or handle.
Who is affected?
The condition appears to be able to affect any breed of horse. Horses are not born with the condition, but develop it, often at the prime of their lives (4-9 years old). Some studies find more geldings affected but others have not found a sex difference.
What should you do if your horse starts to headshake?
If your horse is headshaking badly at rest and appears distressed, then you should contact your vet urgently. If not, then it is worth getting some videos of how and when your horse shakes as this can give important information about possible causes. Your vet can then watch the videos alongside examining your horse.
It is worth seeing if your horse is better with a nose-net on, and if so, how much better. 25% of TGM headshakers are up to 70% better with a nose-net. Of course, this means 75% are not better (some are actually worse) and 70% better is not enough of an improvement if severely affected. Furthermore, not all competitions allow use of a nose-net. However, a nose-net is cheap and non-invasive so the first thing to try. There are broadly 3 different types: one which looks quite like a nose-net, one which is more of a rigid shield and one which is a nose-bag style and it is worth trying all three. Some horses benefit from the use of a face-mask as well as, or instead of, a nose-net. The nose-net is thought to work by constantly stimulating the nerve which helps over-ride pain signals – the same reason you rub your elbow if you bang it and it is less painful, although the damage no different.
A small benefit of supplementing magnesium, which can calm nerve firing, can be expected in TGM headshakers. This is low-risk and sensible as part of a holistic approach but unlikely to be curative.
If these treatments are insufficient and your vet thinks your horse is likely to be a TGM headshaker then the next step, ideally, is referral to an equine hospital with RCVS specialists and a CT scanner. This is the best way to be as sure as possible that TGM headshaking is the diagnosis. Even in a horse which seems very likely from history and observation, to have TGM headshaking, there is a 10% chance of finding another diagnosis at referral.
Treatment
Sadly, because despite best efforts from veterinary researchers, we know very little about how and why TGM headshaking occurs which makes treatment very difficult. Furthermore, even in people, neuropathic pain is notoriously difficult to manage.
If a nose-net and magnesium are insufficient, then EquiPENS neuromodulation, adapted from a management technique used for human neuropathic pain, may be the next treatment to try. Whilst it is low-risk, it is expensive and only available at a few equine hospitals. We can expect a 50% remission (return to ridden work at the previous level) rate but for an unknown and individually variable, length of time (anything from 2 days to 5 years plus). Pharmaceuticals are an option but response is individual and cannot be predicted, it can get very expensive and horses may not compete on the tablets. Sadly, many horses who do not respond to treatment have to be euthanised.
Further information
There is more information, including free webinars, available at Headshaking | B&W Equine Group (bwequinevets.co.uk).
Special thanks to Dr. Veronica Roberts MA(Oxon) MA VetMB(Cantab) PhD PGCert(HE) DipECEIM FRCVS (European and RCVS Specialist in Equine Internal Medicine, Senior Lecturer in Equine Medicine University of Bristol (clinical work at B and W Equine Hospital) and our bursary student Amy Coleman.
Last updated: 23/6/2026. Advice collated by the World Horse Welfare research and education team and externally reviewed by Dr. Veronica Roberts MA(Oxon) MA VetMB(Cantab) PhD PGCert(HE) DipECEIM FRCVS
Share this advice
Popular advice in Health

Mites: how to treat them in horses
Find out how our experienced teams tackle this itchy problem in affected horses and ponies.

Sweet itch
Sweet itch is one of the most common allergic skin diseases affecting horses in the UK - learn how to prevent and manage it.
Other advice categories

All webinar categories:
Call our Advice Line
+44 (0)1953 497 238Not found the advice you were looking for? Our friendly team of horse care experts offer free practical advice. What can we help you with today? Our advice line is available 8.30am-5:00pm, or you can email education@worldhorsewelfare.org.